🧬 Dupilumab: Biologics in COPD
The First Real Paradigm Shift in COPD Care —


The First Real Paradigm Shift in COPD Care — And 👀 Why You Should Read This
Over the last decade, chronic obstructive pulmonary disease (COPD) treatment has quietly undergone a revolution. Not necessarily through the development of new inhalers—but through a redefinition of the pt’s inflammation and how that affects breathing, exacerbations, quality of life (QoL) and treatment.
You see, biologics have been approved for asthma as far back as 2003 (omalizumab), but not until 2023 was there a positive study showing hope specifically for COPD pts. It was in 2024 that the FDA-approved the first biologic for COPD…dupilumab.
This would eventually lead to the Global Initiative for COPD Guidelines (GOLD guidelines) recommending DUPILUMAB as add-on therapy in COPD in 2025.
Also, in 2025, the FDA brought us approval for mepolizumab in COPD.
⭐️ This post will focus on dupilumab.
I’ve created a timeline for you below with the relevant pharma trials.
⚔️ The Biologic Timeline (2015–2025)
| Year | Drug | Target | Outcome |
|---|---|---|---|
| 2017 | Mepolizumab | IL-5 | Hint of benefit in eosinophilic COPD (METREX/METREO), but no approval |
| 2019 | Benralizumab | IL-5Rα | Negative trials (GALATHEA/TERRANOVA) |
| 2023 | Dupilumab | IL-4/IL-13 | Game-changer (BOREAS Trial) |
| 2024 | Dupilumab | IL-4/IL-13 | NOTUS confirms effect; FDA approves |
| 2025 | Tezepelumab / Itepekimab | TSLP / IL-33 | Disappointing or mixed results |
| 2025 | Mepolizubmab | IL-5 | FDA approved based on (MATINEE in NEJM) |
Physiology and Pathophysiology
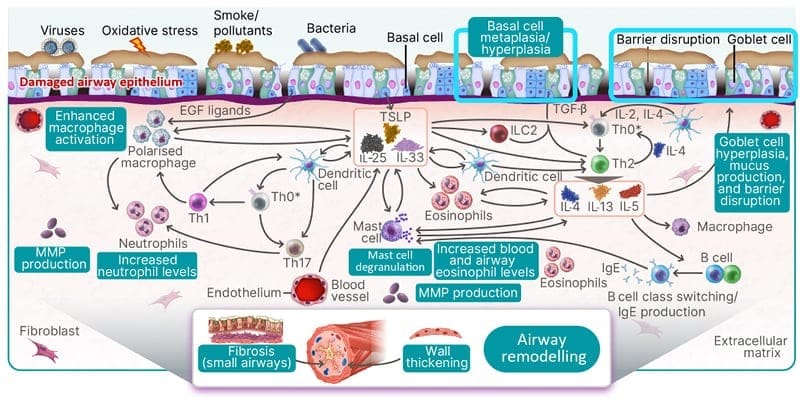
Dupilumab works by blocking interleukins IL-4 and IL-13 pathways in Th2 pathway of airway inflammation.
Normal physiology
IL-4 and IL-13 increase fraction of exhaled nitric oxide (FeNO) and promote eosinophils and type 2 inflammatory cell infiltration into the lung tissues.
COPD Pathophysiology
Those Th2 cell infiltrates lead to airway hyperreactivity, airway remodeling, and fibrosis. They can impair epithelial barrier function. This leads to the mucociliary dysfunction, mucus hypersecretion, and goblet cell hyperplasia.
Th2 inflammation is present in 20-40% of COPD pts. If present, the exacerbation rate is thought to be significant and also thought to be steroid-responsive.
🔬What BOREAS Showed us
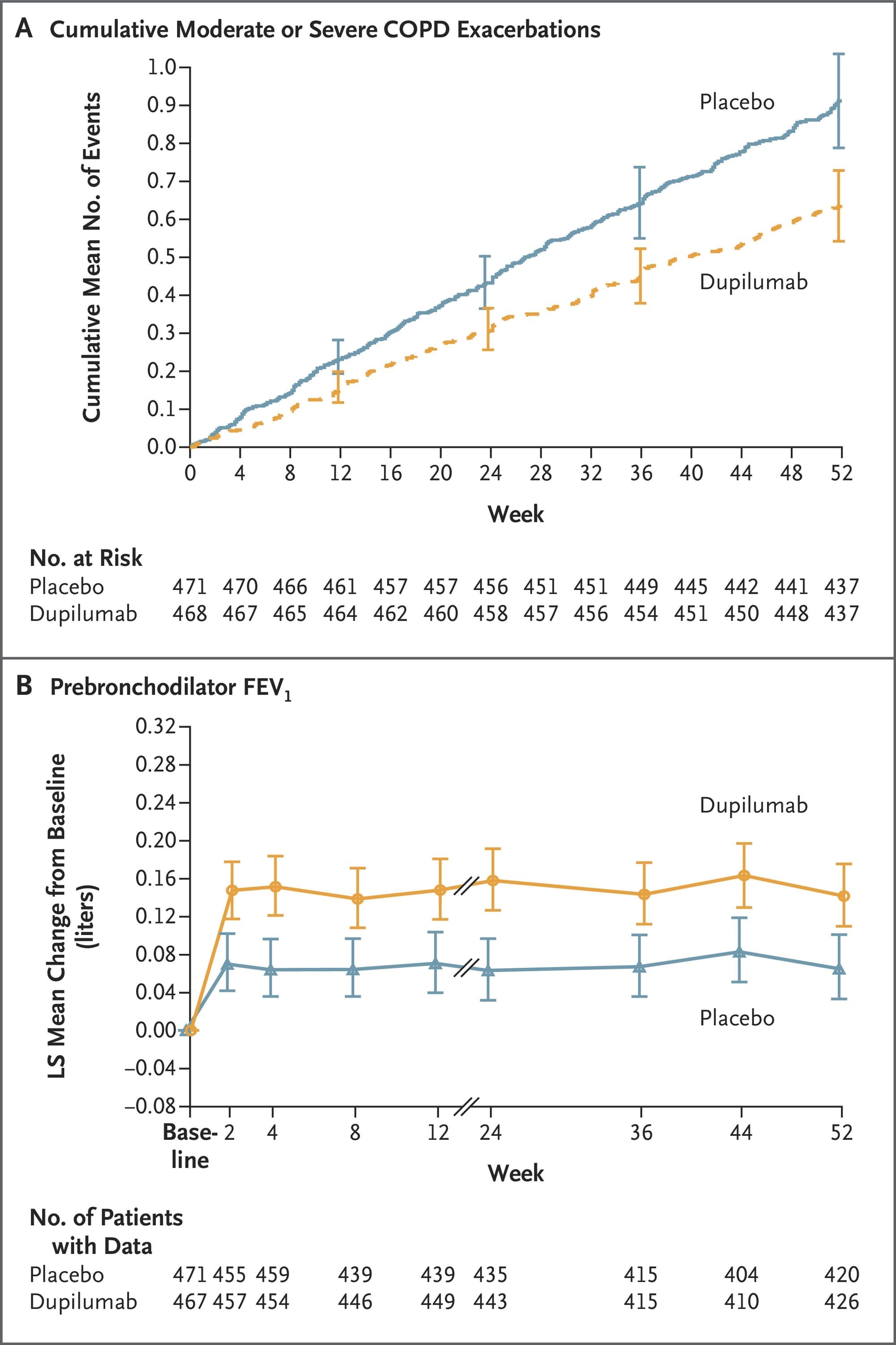
Plot A is showing number of moderate to severe COPD exacerbations each group had over 52 weeks. Placebo had more exacerbations (faster and higher numbers). Dupilumab group showed slower rise meaning fewer total exacerbations per pt, sustained curve separation at week 12, and persistent effect through 1 year. Overall fewer total exacerbations per pt.
Plot B is showing lung function change from baseline at multiple time points. Dupilumab showed rapid and sustained improvement in the forced expiratory volume in 1 second (FEV1) as early as week 2, maintained through week 52. Overall up to 0.20 L improvement. Clinically more like 100 to 150 mL improvement in FEV1.
🧠 Who’s the Right Patient?
You only consider Dupilumab if all of the following are true:
- ≥2 moderate (oral/systemic steroid and/or antibiotic-dependent outpatient) or ≥1 severe (hospitalized) exacerbations in last 12 months
- Already on triple inhaler therapy (ICS + LABA + LAMA)
- Blood eosinophils ≥300 cells/μL (ideally off systemic steroids). Preferably two blood checks over time
- Former smoker or in cessation process
- Chronic bronchitis phenotype or frequent exacerbator
- Adjuncts (azithromycin, roflumilast) have already been considered
🧬 This isn’t for all COPD. It’s for Th-2 COPD — the inflammatory phenotype common among our chronic bronchitis pts.
🛠️ Why Biologics Matter to the Non-Pulmonologist
If you are Hospitalist/ER: Biologics can prevent readmissions. Get ahead of bounce-backs. Flag the right patients.
If you are Cardiology: Th2 inflammation can worsen cardiac outcomes and mimic CHF symptoms
If you are Nephrology: Systemic steroid-sparing strategies matter for the CKD pt.
If you are Palliative/Geriatrics: Better control = fewer crises = better goals-of-care discussions
If you are Primary Care/Internal Medicine/Family Medicine (FP): This is the new era of COPD management — don’t let your patients get stuck in 2010.
🖋️ Prescribe Like a Pro: What to Write, What to Know

Dose: Dupilumab 300 mg SC every 2 weeks
No loading dose for COPD indication. Add to existing maintenance therapy.
📝 Documentation to include for Prior Authorization:
- COPD diagnosis (ICD-10) with ATS/GOLD staging.
- + spirometry
- Inhaler adherence (meds, doses, refill history)
- ≥2 moderate or ≥1 severe exacerbations (dates, oral steroids, ER/hospital)
- Two blood eosinophil counts (BEC) off steroids if available (≥300 cells/µL)
- Adjuncts used (macrolide, PDE4i)
- Smoking/vaccine status
Sample Prior Auth. 👉
"Pt w/severe eosinophilic COPD (BEC ≥300), with ≥2 moderate exacerbations despite triple therapy. Requesting dupilumab 300 mg subcutaneous inj q2week per FDA indication and GOLD 2025."
📈 Pt Follow-Up: When to Check, What to Track
| Timepoint | What to Track |
|---|---|
| 8–12 Weeks | FEV₁, CAT or SGRQ, rescue inhaler use, exacerbation count |
| 6 Months | Look for benefit: fewer flares, improved function |
| 12 Months | No response? Re-evaluate (adherence, phenotype, comorbidities) |
🩺 Potential Pt Adverse Effects:
- Nasopharyngitis
- Conjunctivitis or keratitis
- Fever
- Rash / eczema
- Lymph nodes edema
- EGPA red flags
- Injection-site reactions
- Arthalgia
- Parasitic infections (rare)
📚 Dr Morris: What do the Guidelines Tell Us?
| Guideline | Stance |
|---|---|
| GOLD 2025 | Includes Dupilumab as add-on for eos ≥300, persistent exacerbations |
| NEJM | BOREAS & NOTUS trials confirm benefit |
| ATS / CHEST / ERS | Updates pending?; hopefully to adopt in future iterations |
| SCCM | Not for ICU initiation; outpatient use only |
GOLD, 2025
🔹 Repeat eos counts (off steroids!)
🔹 Don’t de-escalate ICS without good reason
🔹 Biologics are additive — they don’t replace inhalers
🔹 Reassess at 6–12 months — don’t continue blindly
👩🏻🎓 For Boards Study
Dupilumab is the first ever biologic approved for COPD in Sept 2024. It blocks IL4 and IL-13 pathways in the eosinophilic Th2 pathway of inflammation. It is added on top of inhaled triple therapy. It reduces exacerbations and improves FEV1.

🥼Doctor’s Orders
- Confirm: COPD + ≥2 mod/1 severe exacerbations + on triple therapy
- Check BEC ≥300 cells/µL (off steroids if possible)
- Ensure smoking cessation, vaccinations, adjuncts attempted
- Prescribe: Dupilumab 300 mg SC Q2W
- Document: GOLD 2025, BOREAS/NOTUS trial results, eos ≥300, PA language
- Follow: Every 8–12 weeks, reassess at 6 and 12 months
- Stop if no response or intolerant due to adverse effect
🤡 TL;DR
- Dupilumab is a monclonal Ab which blocks/targets type 2 inflammation (via IL-4/IL-13) in eosinophilic COPD.
- This biologic showed fewer exacerbations, better FEV₁, and improved QoL in patients still crashing despite triple inhaler therapy.
- It’s FDA-approved (Sept 2024) and endorsed by GOLD 2025 as add-on therapy.
- Be mindful of adverse effects
📉 The biologic era in COPD has started. But it’s not for everyone — only for those with the right phenotype.
This is not a sponsored post for dupilumab, NEJM, or the GOLD guidelines. I am not affiliated with its makers/authors nor do I speak for them. The views expressed are my own and do not necessarily reflect the views or positions of the above or its affiliates.
📬 Want More Like This?
Upcoming posts:
- 🎯 “The Future? of COPD Biologics: Itepekimab, Tezepelumab & Beyond”
- 💡 “When to Stop ICS in COPD — And When It’s Dangerous”
- 🧠 “The 5 Hidden Endotypes in COPD That GOLD Still Doesn’t Address”
- 😮💨 “ Biologics in Asthma”
🫁 Subscribe and follow @Boka_MD — for quick reads that respect your time, your brain, and your inbox.
💬 Have a case to discuss?
Send it (no PHI please). Comment it. I’ll feature the best ones in future posts.
Let’s keep learning. Together!