Have you ever wondered: WHY a MAP of 65 mmHg?
The 65 mmHg MAP target in critical care medicine has deep historical roots—from Hippocrates’ humors to Poiseuille’s equations.
Here’s the 2nd of the Have You Ever Wondered…? 🧠 series— where we explore the why behind what we do at the bedside.

Today’s question, one I often post to medical students mid-rounds, in between pts, or just in passing:
Why do we use a MAP goal of 65 mmHg in the ICU?
It’s a deceptively simple target. But where did it come from?
Why 65– not 60, not 75?
Let’s go back in time…
And btw…
MAP is defined as mean arterial pressure. It is the average calculated blood pressure during a single cardiac cycle (from vein to relaxed ventricle).
Concept of Shock & Hypotension, and the Birth of Hemodynamic Thinking 💭⚕️
Origins
The earliest known documentation of shock comes from none other than Hippocrates. He used a term he supposedly called exemia — a draining of blood - which he saw as a disturbance in the four humors: blood (sanguine), phlegm, yellow bile, and black bile. Blood, carrying vitality and spirit was central to life.
Losing it was losing life.
The language of “perfusion” was not born yet. Yet the intuition that blood volume and personality were interlinked was already present.
In the 1600s, the idea of circulation began to crystalize. In 1733, Stephen Hales directly measured blood pressure in the arteries - a pivotal moment.
Then came Jean Léonard Marie Poiseuille in 1828. His now-famous equation gave us a framework to understand flow 👇
How is Poiseuille’s Law clinically relevant? 👉
📏 Basically, blood flow is directly proportional to blood vessel’s pressure differences and radius, with an inverse relationship toward viscosity and vessel length.
🤔 In other words, think of vasoconstriction, vasodilation, and increased/decreased red cell counts all affecting flow/circulation.
🫀V̇ = Q = CO = left ventricular cardiac output in cardiac hemodynamics so the formula could be rewritten as such Q = DP/TPR. (DP = driving pressure or MAP - atrial pressure. TPR is total peripheral resistance)
⛔ The equation assumes laminar flow.
So translation?
Blood flow (Q) depends on
- Pressure gradient
- Vessel radius to the 4th power
- Blood viscosity
- Vessel length
This was the beginning of hemodynamic thinking: resistance, tone, viscosity, and pressure were now variables we could manipulate.
Meanwhile:
These were the first inklings that a threshold pressure was necessary for organ perfusion.
And also meanwhile…
The 1900s: Shock, Surgery and Neurophysiology 🔪
1901-1918
Nearly 13 years before World War I, Harvey Cushing identified a key physiological response that would bear his name: the Cushing Reflex.
Simply put, when intracranial pressure (ICP) rises, the body compensates by increasing mean arterial pressure (MAP) to maintain cerebral perfusion pressure (CPP). (Of course, the remaining parts of the triad are irregular breathing and bradycardia.). This discovery was a pivotal early step in the development of neurocritical care.. His work led to the equation below and the MAP equation above.
What is the Cerebral Perfusion Pressure equation? 👉
CPP = MAP - ICP
Where CPP is cerebral perfusion pressure, MAP is mean arterial pressure, ICP is intracranial pressure.
Conceptually, this brings to light the Monroe-Kellie doctrine, which for over 200 years has been a Neurology and Neurosurgical tenet with important clinical basis in understanding the pathophysiology of TBI, stroke, brain cancer/tumor, and even shock patients. The doctrine states that since the skull is a fixed bone structure, its combined contents have fixed volume — the neuronal tissue, blood within the Circle of Willis, Circle itself, and the cerebrospinal fluid may create opposition if any one piece of the equation increases or decreases in volume. Interestingly, though, in recent years, this doctrine has been called into revision…
(CVP can also interchange with ICP)
What is considered normal CPP? 👉
Normal CPP lies between 60 and 80 mmHg.
So what is normal ICP? 👉
If CPP is considered within normal range of 60 to 80 mmHg, then intracranial pressure or ICP should be within 5 to 10 mmHg.
ICP can be measured directly by intracranial pressure transduction.
Yet it was the trauma survived on the battlefield by the end of the first world war which led to studies confirming MAP <60 mmHg leads to irreversible shock.
👉 So at this point in the timeline it’s the year 1918 when we actually have the threshold of 60 mmHg.
Recall this👇 fun diagram from cardio phys?
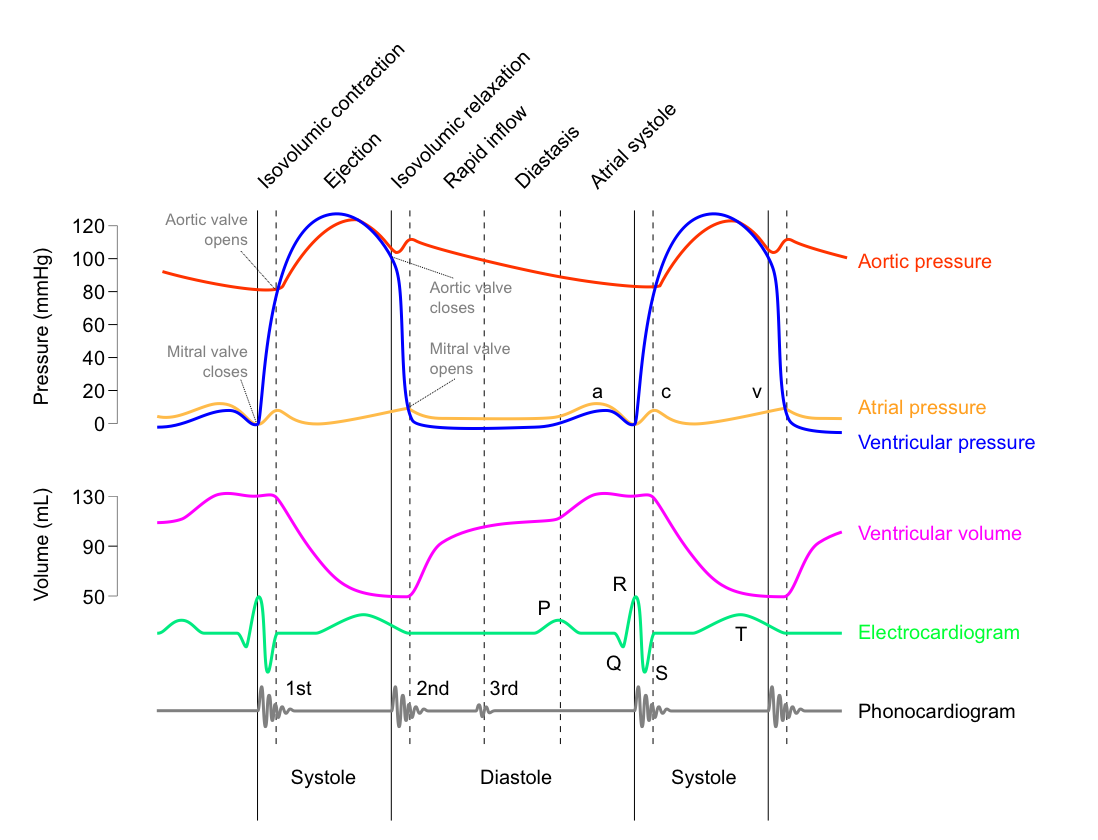
Absolutely, you do. That’s the famous Wiggers Diagram.
Thus Carl Wiggers ties perfusion pressure directly to survival in shock.
Fast-forward to 1970s for Shubin:
This categorization of shock states emphasized MAP as the clinical anchor.

Next step in our timeline is the modern area. But before we approach this, we need to look at a key trial called SEPSISPAM.
The SEPSISPAM Trial (2014)
Personalizing the Target?
Published in the New England Journal of Medicine, the SEPSISPAM trial was a pivotal RCT that randomized 776 patients with septic shock to either:
• Low MAP target (65–70 mmHg)
• High MAP target (80–85 mmHg)
Primary outcome? 28-day mortality.
Result? No significant difference overall.
But there was a key subgroup signal:
In patients with chronic hypertension, a higher MAP (80–85 mmHg) was associated with less need for renal replacement therapy.
This supported the hypothesis that patients with shifted autoregulatory curves—like those with long-standing hypertension—might require higher perfusion pressures to adequately perfuse vital organs.
The trial confirmed:
• 65 mmHg is adequate for most pts
• Some patients may benefit from individualization—especially when it comes to renal perfusion and chronic vascular tone.
Modern Era 📱
Goal-Directed Therapy & Guidelines
Okay, finally, we are at the end of this timeline. Finally making sense, right?
We have some hundreds of years of pioneering background leading up to validated trials supporting this MAP threshold of 65mmHg. Here are the important remaining pieces:
Dr. Rivers’ Early Goal-Directed Therapy (EGDT) trial in 2001 set off a revolution. For the first time, MAP ≥65 mmHg was codified as a central endpoint in septic shock resuscitation.
Subsequent trials—ProCESS, ARISE, and ProMISe—were unable to replicate EGDT’s mortality benefit yet they upheld early recognition of sepsis, early use of antibiotics, and also upheld MAP ≥65 mmHg as a safe, default threshold.
The Surviving Sepsis Campaign and SCCM/CHEST guidelines adopted 65 mmHg as the standard MAP target in shock, citing both safety and simplicity.
The Surviving Sepsis Campaign (SSC), which includes the Society of Critical Care Medicine, European Society of Intensive Care Medicine (ESICM), recommends targeting a MAP of 65 mm Hg for initial resuscitation in patients with septic shock requiring vasopressors.
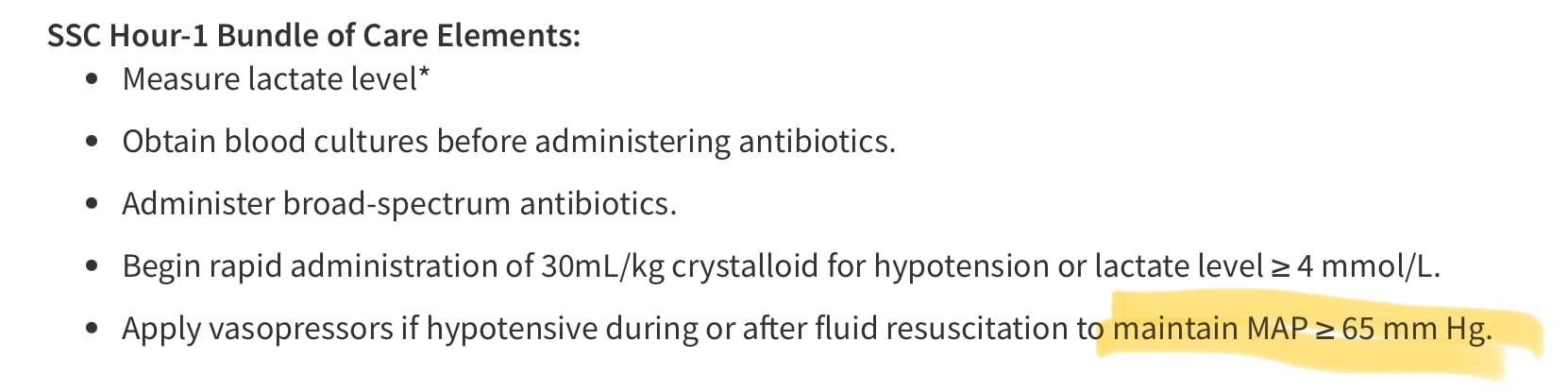
Tap for 2021 SSC Guidelines from SCCM
But What About Higher or Lower Targets? 🎯
A 2023 meta-analysis by Carayannopoulos et al. pooled RCT data to compare:
• High MAP targets (75–85 mmHg)
• Standard MAP (65 mmHg)
• Permissive hypotension (60–65 mmHg)
Findings:
• No mortality benefit with higher MAPs
• No harm with permissive hypotension in selected patients
• Chronic hypertensives may benefit from higher MAP (echoing SEPSISPAM)
Doctor’s Order 🥼
Final Thoughts
So…if you made it through to the end of this, then you can see that 65 mmHg is our Goldilocks number:
• Not too low to risk organ ischemia
• Not so high as to provoke adverse events (e.g., tachyarrhythmias, vasopressor burden)
The history and curiosity within medicine is fascinating. Let us go back and review and recall the journeys of past advancements and the people who got us here.
Let this post serve as both a journey through history and a reminder:
Behind every goal or target at the bedside lies a century-spanning arc of physiology, war, trauma, and trial.
TL;DR 🤡
- The 65 mmHg MAP target has deep historical roots—from Hippocrates’ humors to Poiseuille’s equations.
• MAPs <60 mmHg have been repeatedly linked to renal and cerebral ischemia.
• The Cushing Reflex and Monro-Kellie Doctrine showed that perfusion pressure matters, especially in neurocritical care.
• 20th-century trauma and shock physiology reinforced the threshold of 60–65 mmHg.
• The SEPSISPAM trial confirmed that while 65 mmHg is safe for most, hypertensive patients might benefit from MAPs of 80–85 mmHg to protect renal function.
• Modern guidelines and RCTs support 65 mmHg as a safe, effective, and pragmatic default.
- Read the journals lol.
References
Harvey, W. Exercitatio Anatomica de Motu Cordis et Sanguinis in Animalibus. 1628.
Hales, S. Haemastaticks, Philosophical Transactions of the Royal Society, 39(2), 57-90. 1733.
Manji et al. The History and Evolution of Circulatory Shock. Critical Care Clinics, January 2009, pp1-29.
Poiseuille, J.L.M. Recherches sur la force du cœur et sur les effets des saignée. Annales de Chimie et de Physique, 37, 3-58. 1828.
Sutera et al. The History of Poiseuille’s Law. Annual Rev. Fluid Mech. 1993; 25.
Ludwig, C. Beiträge zur Kenntniss des Einflusses dear Respirationsbewegungen auf den Blutlauf im Aortensysteme. Archiv für Anatomie, Physiologie und Wissenschaftliche Medicin, 16(1), 242-302. 1847.
Bernard, C. Leçons sur les phénomènes de la vie communs aux animaux et aux végétaux. 1878.
Benson et al. The Monro-Kellie Doctrine: A Review and Call for Revision. AJNR Am J Neuroradiol. 2023 Jan;44(1):2–6. doi: 10.3174/
Wiggers, C.J. Physiology of Shock. 1937.
Mean Arterial Pressure Targets and Patient-Important Outcomes in Critically Ill Adults: A Systematic Review and Meta-Analysis of Randomized Trials. Carayannopoulos KL, Pidutti A, Upadhyaya Y, et al. Critical Care Medicine. 2023;51(2):241-253. doi:10.1097/CCM.0000000000005726.
Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M; Early Goal-Directed Therapy Collaborative Group. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001 Nov 8;345(19):1368-77. doi: 10.1056/NEJMoa010307. PMID: 11794169.
Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, Machado FR, Mcintyre L, Ostermann M, Prescott HC, Schorr C, Simpson S, Wiersinga WJ, Alshamsi F, Angus DC, Arabi Y, Azevedo L, Beale R, Beilman G, Belley-Cote E, Burry L, Cecconi M, Centofanti J, Coz Yataco A, De Waele J, Dellinger RP, Doi K, Du B, Estenssoro E, Ferrer R, Gomersall C, Hodgson C, Møller MH, Iwashyna T, Jacob S, Kleinpell R, Klompas M, Koh Y, Kumar A, Kwizera A, Lobo S, Masur H, McGloughlin S, Mehta S, Mehta Y, Mer M, Nunnally M, Oczkowski S, Osborn T, Papathanassoglou E, Perner A, Puskarich M, Roberts J, Schweickert W, Seckel M, Sevransky J, Sprung CL, Welte T, Zimmerman J, Levy M. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021 Nov;47(11):1181-1247. doi: 10.1007/s00134-021-06506-y. Epub 2021 Oct 2. PMID: 34599691; PMCID: PMC8486643.
Asfar P, Meziani F, Hamel JF, Grelon F, Megarbane B, Anguel N, Mira JP, Dequin PF, Gergaud S, Weiss N, Legay F, Le Tulzo Y, Conrad M, Robert R, Gonzalez F, Guitton C, Tamion F, Tonnelier JM, Guezennec P, Van Der Linden T, Vieillard-Baron A, Mariotte E, Pradel G, Lesieur O, Ricard JD, Hervé F, du Cheyron D, Guerin C, Mercat A, Teboul JL, Radermacher P; SEPSISPAM Investigators. High versus low blood-pressure target in patients with septic shock. N Engl J Med. 2014 Apr 24;370(17):1583-93. doi: 10.1056/NEJMoa1312173. Epub 2014 Mar 18. PMID: 24635770.



{kind=link}