Have you ever wondered: WHY do we reach for Sodium Bicarbonate in the ICU?

A History, A Physiology, A Philosophy
My apologies to this growing readership. After taking the summer of 2025 off from blogging, I’m back. I appreciate your patience 😀.
Let’s try a new take today— I’ll attempt to weave history, physiology, evidence, controversy, and philosophy into a practical piece.
Here is #3 of the Have You Ever Wondered…? 🧠 series- where we explore the why behind what we do at the ICU bedside.

Today’s question:
Why do we reach for sodium bicarbonate in the ICU?
🌙 👩⚕️🏥
Okay, let’s say it’s 3:00 a.m. in the ICU.
A patient lies before you: blood pressure collapsing, lactate rising, arterial blood gas pH of 6.9. The nurse asks: “Should we start a bicarb drip?”
Well, let’s just say, few questions in critical care stir more debate than this one. Sodium bicarbonate — one of the oldest drugs in our armamentarium — sits on the shelf, deceptively simple, almost alchemical: a white powder that promises to neutralize the acid of death itself. But behind that small vial lies more than a century of history, a web of physiology, and a philosophy of medicine that stretches back to antiquity.
A History: Brief Origins to Modern ICU
🏥
Bicarbonate, first crystallized by French chemists in the 18th century, was not born as an ICU drug. Look up the Leblanc process (salt to soda ash, precursor process to making sodium bicarbonate) if you are interested. (Some web searches suggest ancient Egyptians first started with natron, a naturally occurring compound salt.)
Overall though, bicarb, as we call it, began in kitchens and factories as baking soda. In medicine, its journey started with treating “acid stomachs,” moved through resuscitation attempts in World War II field hospitals, and found its way into the ICU as a reflexive antidote to lactic acidosis in the 1960s and 70s.
But as modern physiology emerged, voices grew skeptical. By the 1980s, intensivist- and nephrologist-talking heads argued that bicarbonate was too blunt a tool — shifting carbon dioxide across cell membranes, perhaps worsening intracellular acidosis.
So, was it salvation, or illusion?
A Physiology: The Dance Between Acid and Base
🔛 🔙♾️
At its core, sodium bicarbonate (NaHCO₃) does one thing: it buffers hydrogen ions. It reacts with H⁺ to form H₂CO₃, which dissociates into water and CO₂.
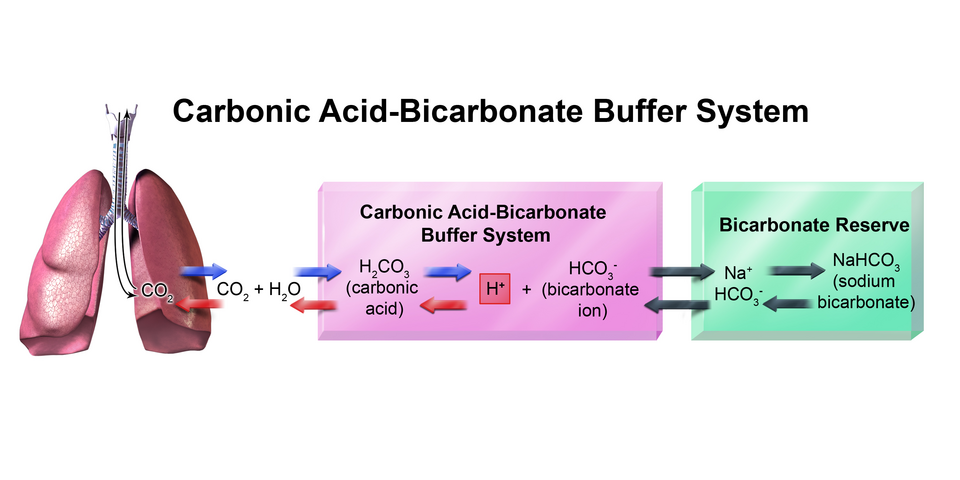
Key physiological consequences:
- Immediate effect: rises in serum pH and HCO₃⁻, often stabilizing cardiac contractility and catecholamine responsiveness.
- Downside: the CO₂ ion produced diffuses rapidly into cells and across the blood–brain barrier, potentially worsening intracellular acidosis if ventilation cannot keep up.
In the lung 🫁, this means you must have a ventilation system ready to sweep away the exhaled CO₂. In the kidney 🫘, it means shifting sodium and water loads. In the brain, it means the possibility of paradoxical worsening — a cruel irony.
Pharmacokinetically, sodium bicarbonate distributes rapidly in extracellular fluid, with renal excretion dependent on GFR, and with sodium load implications for heart failure and volume-sensitive patients.
The Evidence: Trials & Guidelines
📑🔬
For decades, we had dogma, not data. Then came trials.
- No benefit in lactic acidosis: Studies since the 1980s onward showed that routine bicarbonate in sepsis, elevated lactic acid, and lactic acidosis did not improve mortality or hemodynamics (Cooper et al., 1990).
FANTASTIC MODERN READ ON LACTATE & THE LACTATE SHUTTLE
Paper by George A Brooks:
- The BICAR-ICU Trial (2018, JAMA): In 389 patients with severe metabolic acidosis (pH ≤7.20, HCO₃⁻ ≤20), sodium bicarbonate did not improve the primary composite outcome overall. (Mortality and organ failure.) But in the pre-specified subgroup of patients with acute kidney injury, bicarbonate reduced the need for dialysis and improved survival【PubMed ID: 29946726)].
- Cardiac arrest: The AHA and European Resuscitation Council recommend against routine bicarbonate during CPR, reserving it for special circumstances (e.g., hyperkalemia, tricyclic antidepressant overdose, severe pre-existing metabolic acidosis).
Name 3 circumstances in cardiac arrest where sodium bicarbonate use is supported by societies. 👉
- Hyperkalemia
- Tricyclic antidepressant overdose
- Severe pre-existing metabolic acidosis
- DKA: Guidelines emphasize insulin and fluids first; bicarbonate is only indicated if pH <6.9, reflecting the dangers of hypokalemia and paradoxical CNS acidosis. Some sources even argue that <7.05.
🌍 International guidelines today (SCCM, ESICM, KDIGO):
- Do not use bicarbonate routinely for lactic acidosis in sepsis.
- Consider it when pH <7.1, especially with concomitant AKI.
- Use it for specific toxicologic indications (TCA overdose, salicylate poisoning, hyperkalemia with ECG changes).
- NAGMA (Non-anion gap metabolic acidosis) with a serum bicarbonate level usually less than 18 mEq/L could be considered for exogenous bicarbonate administration.
A Philosophy: Controversy & Conceptual Discord
💬
Why So Much Controversy? 🗣️
I think we can say this because bicarb sits at the intersection of numbers and narrative.
3 P’s:
- On paper: It raises pH.
- In physiology: It can worsen intracellular acidosis.
- In practice: Sometimes it saves the crashing patient long enough for definitive therapy.

But it‘s a drug of temporality…it buys time— yet does not cure disease. Like a sorcerer’s stone, it can appear to transmute crisis into stability, but at a cost.

The controversy endures because clinicians are haunted by two fears:
- Doing nothing while a patient acidifies into arrest.
- Doing harm by chasing numbers with chemistry instead of physiology.
Philosophy at the Bedside
Marcus Aurelius: “What stands in the way becomes the way.”
Acidosis is not merely a lab value— it is a signal of failing cellular respiration, of mitochondria gasping under hypoxia, sepsis, or shock. To treat only the number is to miss the message.
Yet, philosophy also teaches pragmatism: when the patient’s heart is failing at pH 6.9, due to the extensive acidic milieu, even a temporary reprieve may give time for antibiotics, fluids, or dialysis to take hold. Bicarb, then, is less a cure and more a bridge — a plank laid across the torrent.
Doctor’s Order 🥼
Final Thoughts
When to consider bicarb:
✅
- Severe metabolic acidosis (pH <7.1) with AKI or impending need for RRT/dialysis.
- Tricylic antidepressant (TCA) overdose
- Hyperkalemia
- Salicylate (aspirin) toxicity
- DKA with pH <6.9
- Specific peri-arrest scenarios, guided by ACLS: hyperkalemia, above
When to avoid bicarb:
🚫
- Routine use in lactic acidosis from sepsis/shock.
- Isolated hyperchloremic metabolic acidosis without severe acidemia.
- Patients with volume overload, uncontrolled ventilation, or risk of hypernatremia.
Physician/APP Pearls:
🩺
- Bolus (1–2 mEq/kg) for immediate rescue.
- Infusion (commonly 150 mEq in 1L D5W over several hours) for ongoing acidemia, guided by blood gases.
- Always consider to pair with adequate ventilation to eliminate excess pCO₂.
- Monitor electrolytes: potassium, calcium, sodium shifts.
- Monitor pH.
Nursing/RT Pearls:
👩⚕️🧑⚕️💉
- Watch for peripheral IV extravasation— sodium bicarbonate is caustic.
- Auscultation for crackles— sodium bicarbonate can cause pulmonary edema.
- Track ABGs closely as not to overcorrect.
- Document hemodynamic response, urine output, neuro status/exam.
🤌🏼
Sodium bicarbonate is not a panacea. It is not the sorcerer’s stone. It is, rather, a reminder: that in critical care, numbers on a blood gas are both truth and illusion. The truth is acidemia kills. The illusion is that neutralizing the acid is the cure.
We reach for bicarbonate not because it solves the problem, but because sometimes it buys us time to solve the problem.
And in the ICU, time is often the most precious drug of all.
Maybe one day precision medicine will hit our Units. Mitochondrial dysfunction will be targeted in critical illness the way we are now targeting neoplastic cells by sophisticated immunotherapy.
TL;DR 🤡
- History: Bicarb started as baking soda → field resuscitations → reflex ICU therapy
- Physiology: Buffers H⁺, raises pH, but generates CO₂ → risk of paradoxical intracellular acidosis if ventilation is inadequate.
- Evidence:
- No benefit in routine lactic acidosis/sepsis
- BICAR-ICU Trial (2018): No overall survival benefit, but improved outcomes in patients with AKI
- Supported in cardiac arrest only for hyperkalemia, TCA overdose, or severe pre-existing acidosis.
- DKA: Only if pH <6.9.
- Guidelines (SCCM, ESICM, KDIGO):
- Don’t use it reflexively.
- Consider when pH <7.1, especially with AKI or toxicology emergencies.
REFERENCES
Kraut JA, Madias NE. Lactic Acidosis. N Engl J Med. 2014;371(24):2309–2319. PMID: [25494270].
Brooks, GA. Lactate as a fulcrum of metabolism. Redox Biology. 20-20 August, volume 35, 101454.



{kind=link}