Have You Ever Wondered Why Sepsis Patients Crash So Quickly?
Sepsis doesn’t usually announce itself loudly at first. It holds itself together until it can’t.

Have You Ever Wondered Series: BOKA on Medicine, Meaning, Living. This Teaching Edition looks closely at sepsis physiology and the moment compensation gives way. Also published at BokaMD.substack.com.
“Any man’s death diminishes me, because I am involved in mankind.” - John Donne from Meditations XVII from Devotions upon Emergent Occasions, 1624.
Sepsis is one of those ICU conditions that makes you feel like you are watching a human being tip over in real time. Sometimes it happens in slow motion, a gradual loss of footing you can almost narrate. Sometimes it happens all at once.
That patient with pneumonia is sitting up, talking, even joking a little, finishing breakfast. They apologize for bothering the nurse. Their pressure is fine. Their skin is warm. Someone says, “They do not look that bad. Why are they still in the Unit?” And you feel the pull of the numbers, because the monitor is calm and the vitals look reassuring.
So you do what experienced clinicians do. You keep watching. You listen to the room. You track the small things. You know stability is more than a cuff pressure and a single snapshot of vitals.
But you also anticipate. A seasoned clinician anticipates what is coming next and acts accordingly.
Then the nurse calls. Something has shifted. Not just a number. The patient is different. It’s a feeling. And if you’ve been doing this long enough, you know exactly what that feels like — the moment when the hair on your arms rises before your brain has found the words.
Have you ever wondered why sepsis patients do not slide downhill gradually, but seem to step off a ledge?
This is not random. It is physiology. More precisely, pathophysiology. It is the body showing early signs that its internal agreements are starting to fail.
Sepsis Is Not Just an Infection Problem.
You see, we define sepsis as infection with a systemic response, but the danger is rarely the microbe alone. It is the response. A defense system meant to be precise becomes imprecise, and the body’s micro-machinery begins to unravel.
The endothelium, that thin, intelligent inner lining that keeps blood where it belongs, becomes inflamed and porous. Fluid leaks into spaces where it does not belong. Vascular tone softens. Resistance falls.
That is why a patient can look okay and still be quietly losing ground.
A Brief History We Still Carry With Us
Long before bundles and definitions, Avicenna described febrile illnesses that spread beyond the initial source, reaching a point where the entire host was involved. He did not have lactate or vasopressors, but he recognized the same turning point we still recognize today: when an illness stops being local and becomes systemic.
After nearly 2,000 studies and trials on PubMed, our era tried to make sepsis tangible.
Yet, in the end, Dr. Rivers was right about
: Early recognition.
: Timely antibiotics.
: Good resuscitation.
Everything else was commentary (well, except maybe the glycocalyx). New definitions added biological nuance, but they did not change the moment that decides outcomes: when we notice, and when we act.
And even now, the field keeps nudging us back toward the bedside.
One of the most useful “recent” reminders came in 2025 with ANDROMEDA-SHOCK-2, a large randomized trial that focused on a simple, human measurement (capillary refill time) as a resuscitation target in early septic shock, and asked whether tailoring care around perfusion at the skin might outperform our usual habits.
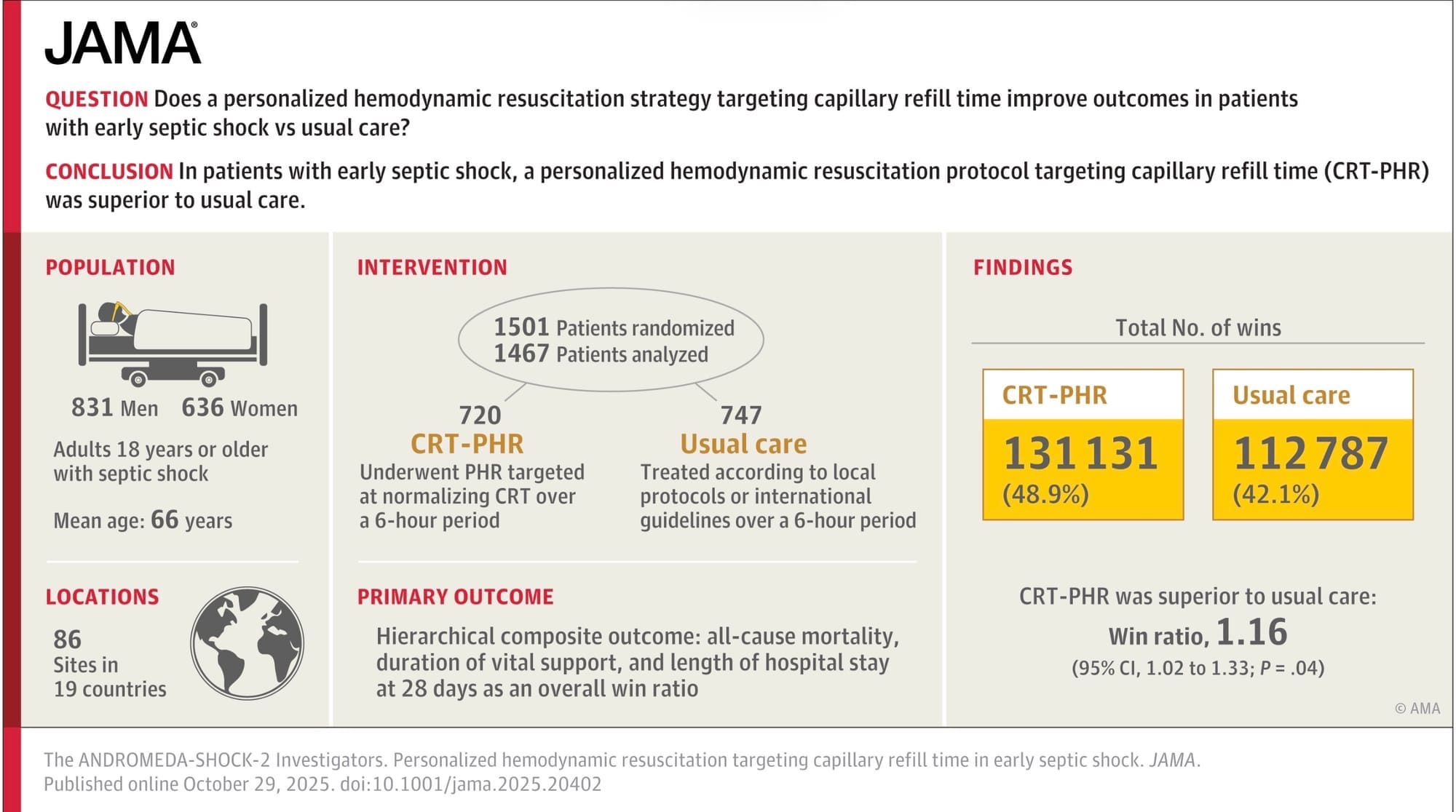
(Whatever your take on the details, it’s a meaningful signal that sepsis care is still circling back to the microcirculation, not just the macro numbers.)
The Lie of “Normal” Numbers
We love numbers because they feel clean.
MAP 65. Heart rate 102. Oxygen saturation 96%.
But sepsis often declares itself first in the microcirculation. Capillaries clog. Flow becomes uneven. Some tissues receive plenty, others almost nothing. It is like a city where the highways are open but the side streets are blocked. From a distance, everything looks fine. Up close, entire neighborhoods are cut off.
For you Seinfeld nerds out there:
“Serenity now… insanity later!”
That is compensation. The body holds its composure, until it can’t. It keeps a straight face until it can’t. That is why mentation changes early. Why urine slows. Why the skin tells the truth before the blood pressure cuff does.
When Oxygen Flows but Can No Longer Be Used
Sometimes oxygen arrives and cannot be used by the cell. Inflammation disrupts mitochondrial function. Cytopathic dysoxia.
Energy production becomes inefficient. Cells shift into survival mode. Lactate rises not only because delivery is impaired, but because utilization is impaired.
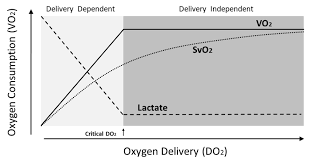
The lights are on. The fuel is there. The micromachinery is faltering? Well, it is faltering.
Why the Crash Feels Sudden
Sepsis is not a linear cascade of events. The body compensates until it cannot. Small losses accumulate quietly until a threshold is crossed, and then buffering collapses fast.
That is why a nurse can say, “He was fine an hour ago,” and be right. He was.
Until he was not.
What Is Really Happening at the Bedside
When we treat sepsis, we are racing against the clock. We need time.
Time for antibiotics to work. Time for inflammation to settle. Time for the microcirculation to reopen. Time for cells to find their micromachinery and rhythm again.
Fluids, pressors, oxygen, ventilation — none of these are definitive cures. They are what I call bridges.
And in the ICU, bridges are of the highest value. They carry someone across a stretch they cannot cross alone.
Doctor’s Order
At the end of the day, protocols matter. Speed matters. Time matters.
But beneath all of that urgency is a quieter truth: sepsis is the body unraveling against its will. Not in a straight line. Unapologetically.
It compensates, compensates, compensates…and then it crosses a threshold, and the whole system stops being able to pretend.
So when a septic patient crashes quickly, it is not always a failure of vigilance. Sometimes it is simply the nature of the physiology. The body holds its composure until it can’t.
That is the real work at the bedside: recognition. Awareness. The ability to feel the nonlinear cascade before the numbers give you permission. To anticipate. To move early. To build time.
Because in sepsis, that is what we are always trying to create: time for antibiotics to work, time for perfusion to return, time for cells to restart their micro-machinery.
And our job, together, is to respond with timeliness, steadiness, teamwork, and clarity…and to build enough bridge to get them to the other side.