The Lingering Cough
Have you ever wondered why coughs outlast colds? Studies shows that post-infectious cough persists in approximately 25% of patients with upper respiratory infections, sometimes for up to two months after the initial illness has resolved.
#DeepDive #Physiology
Have you ever wondered why coughs outlast colds?
Part 1 of the “Have You Ever wondered…” Series
I‘m kicking off a new post series called “Have You Ever Wondered Why…” —where I explore fascinating medical and scientific questions that may have crossed your mind but never made it to Google.
I hope this will be a thought-provoking and intellectually stimulating journey for both of us. Tell me what you think in the comments below! ⬇️

Have You Ever Wondered
why coughs outlast colds?
Why does that "simple cold" leave you with a nagging cough for weeks or even more?
It most likely has happened to you.
As a lung doctor, I see this frustratingly common scenario in clinics daily, and yet I am not always asked why this occurs. As patients, many of us have experienced it firsthand.
In the clinic, I usually explain that traditional teaching supports that your cough will linger for approximately 6-8 weeks after you have completed a respiratory illness.
Observationally, I feel this is just as true for lower respiratory tract infections.
But why is this?
The Cough Arc Reflex
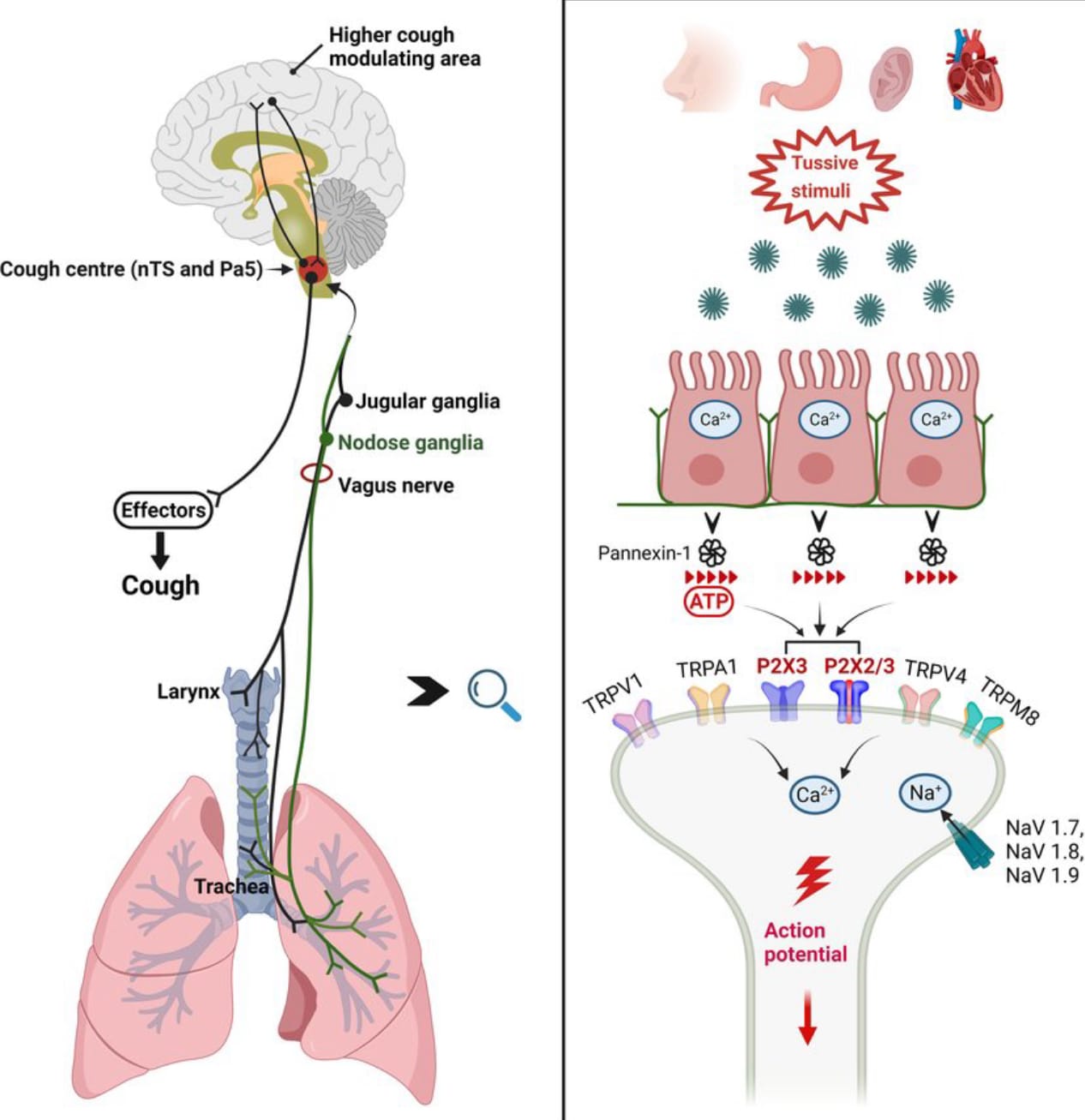
Much has been written about the cough reflex. It’s a fascinating arc of which I plan to discuss the “how of cough” in another post. For now, just review the 6 steps below so we can get into the why of lingering.
6 defined steps of the cough reflex arc:
🦠 🔄🫁🔄🧠🔄🩻🔄🗣️
- Irritant stimulation of cough receptors
- Afferent signal transmission via vagus nerve
- Central processing in the medulla's cough center
- Efferent signals to respiratory muscles
- Coordinated muscle contraction
- Cough production and expectoration
From Cough to Cilia
That was the cough arc, and it’s a complex doozy of physiology in itself.
To get to cough, we need a trigger (an insult), if you will.
Let’s start with a viral infection.
When a viral infection hits your precious respiratory epithelium, it triggers a cascade of events that can long outlast the virus itself.
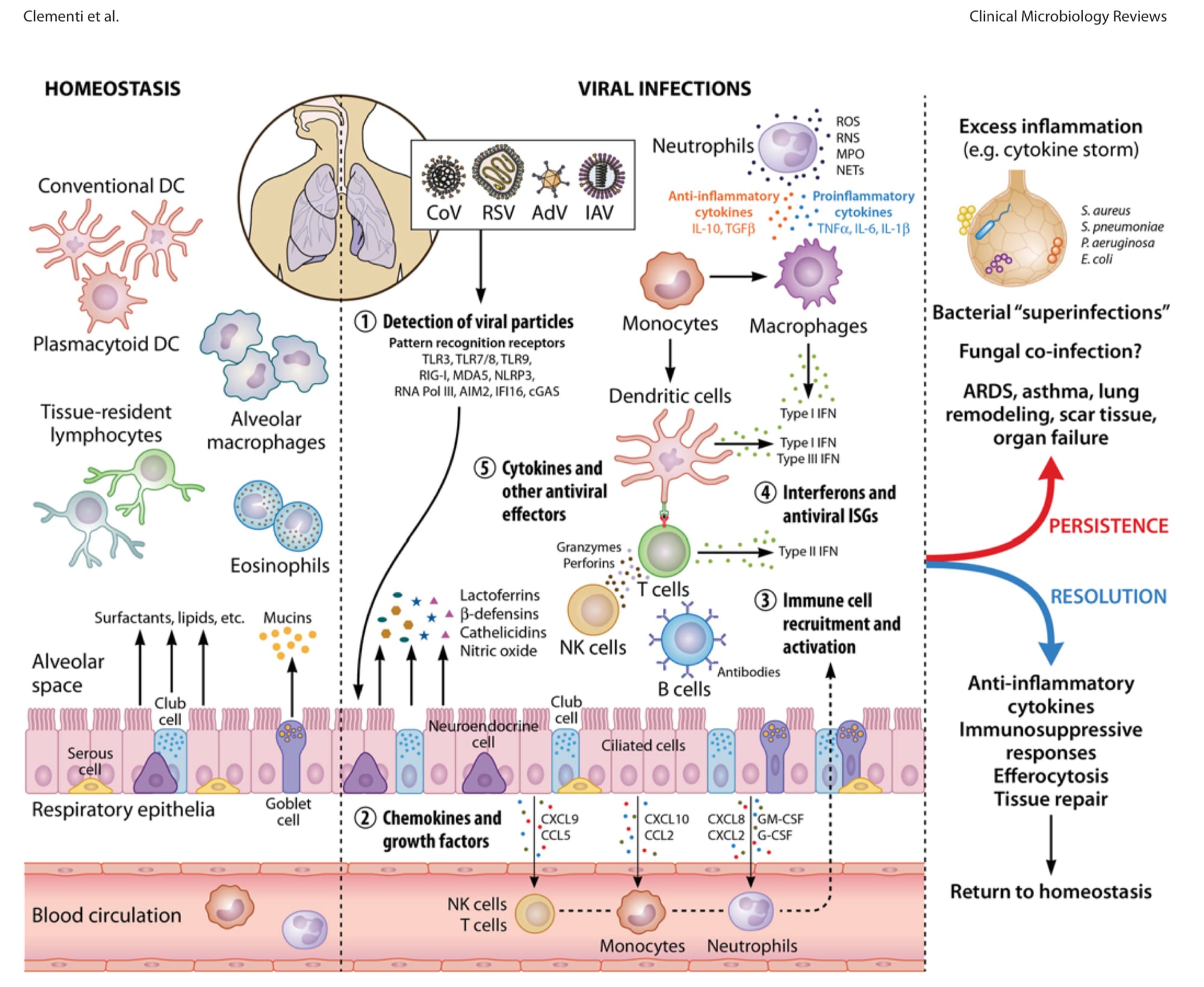
The viral particle(s) exert direct damage to the respiratory epithelium…this leads to disruption of the mucociliary escalator, one of the two major parts of our pulmonary hygiene mechanism (the second obviously being coughing).

It has been studied that the bronchial cilia which beat upward to remove the mucin, can shorten, derange, become saturated, or simply become stunned.

In some cases, adult airways become overly stimulated and sensitive - a term coined to be cough hypersensitivity syndrome. The cough reflex essentially develops a lower threshold, making cough in response to stimuli that wouldn't normally trigger one. Allotussia fits into this syndrome.
Regeneration of this insulted epithelium takes time, often 6-8 weeks for complete restoration!
Deeper Dive:
Physiological Explanations
But let’s really try to under why coughs linger.
You see, the persistence of cough after viral infection involves sophisticated neural and inflammatory mechanisms that unfold in several phases:
🦠 Initial Epithelial Injury & Inflammatory Cascade
- Respiratory viruses (rhinovirus, coronavirus, influenza, etc.) infect airway epithelial cells by 1️⃣ triggering epithelial cell death through both apoptotic and necrotic ☠️pathways, and 2️⃣ causing epithelial damage by exposure of delicate and sensory nerve endings in the submucosa (which are normally protected from environmental stimuli). 😳
- the damaged cells release damage-associated molecular patterns (DAMPs) and pro-inflammatory cytokines—particularly IL-1β, IL-6, IL-8, and TNF-α—initiating a robust inflammatory response. These cytokines directly sensitize the TRPV1 and TRPA1 receptors on vagal afferent nerves, lowering the activation threshold of these cough sensors.
😰Neurogenic Inflammation & Neural Plasticity
Beyond direct viral damage, the cough persistence involves neurogenic inflammation. Exposed sensory C-fibers and Aδ-fibers in the airways release substance P and neurokinin A when stimulated. These neuropeptides trigger:
- Local vasodilation and increased vascular permeability 🥵
- Recruitment of inflammatory cells (neutrophils, eosinophils, macrophages)
- Mast cell degranulation, releasing histamine and prostaglandins🤒
- Stimulation of goblet cells to produce excess mucus 🤧
Mechanistically, this occurs through changes in ion channel expression (particularly TRP channels and voltage-gated sodium channels) and alterations in gene expression within vagal sensory neurons, creating a state of heightened excitability.
⛓️ Neuronal Central Sensitization
The persistent bombardment of sensory input from hypersensitive peripheral nerves leads to central sensitization—changes in the brainstem's nucleus tractus solitarius (NTS) where these afferents synapse.
- Electrophysiological studies have shown increased synaptic strength and reduced inhibitory control in these central pathways following respiratory viral infections.
This central sensitization explains why some patients develop hypersensitivity not just to specific irritants but to thermal changes (cold air), mechanical stimulation (talking, laughing), and even non-respiratory triggers.
🫀Autonomic Nervous System Dysregulation
Post-viral cough often involves autonomic nervous system imbalance. The tonic inhibitory effect of the parasympathetic system on airway sensory nerves becomes impaired. Simultaneously, sympathetic upregulation contributes to bronchial hyperresponsiveness through altered β2-adrenergic receptor function.
Heart rate variability analysis has shown persistent autonomic dysfunction in patients with post-viral cough, showing decreased parasympathetic tone correlating with cough severity scores.
🏗️. Epithelial Remodeling & Repair Dynamics
The rebuilding of airway epithelium follows a highly regulated sequence:
Days 1-3
- Migration of adjacent epithelial cells to cover exposed basement membrane
Days 3-14
- Proliferation of basal cells and transit amplifying cells
Days 14-28
- Differentiation into specialized epithelial cell types
Days 28-56
- Complete ciliation restoration
During this repair phase, transitional epithelium still lacks the tight junctions and barrier function of healthy epithelium.
Single-cell RNA sequencing has recently identified distinct transcriptional signatures during this repair process, with abnormalities in the KGF/FGFR2b signaling pathway associated with delayed epithelial restoration and prolonged cough.
🧠 💉Neuroimmune Interactions & Resolution Failure
In persistent post-viral cough, there's evidence of failed resolution mechanisms. Specialized pro-resolving mediators (SPMs) like resolvins and protectins, which normally terminate inflammation, show reduced expression in patients with prolonged symptoms.
The neuronal-immune cell crosstalk becomes dysregulated, creating a feed-forward cycle where sensory nerve activation maintains immune cell recruitment, which in turn sensitizes nerves through mediator release—a vicious cycle driving symptom persistence beyond the active infection phase.
The Nighttime Nuisance:
Why Coughs Worsen After Dark
Well, okay THAT was complicated.
But that’s it. THAT’s why it takes forever (apparently “56days-forever”) to get over that cough.
But what about those nighttime symptoms??
Many patients report their lingering cough becomes dramatically worse at night.
Those nocturnal exacerbations have several evidence-based explanations:
🧘♀️Postural changes affect mucus drainage:
- When we lie down, mucus that normally drains down the back of the throat with gravity can pool, triggering the cough reflex.
🌞🌝 Circadian variation in bronchial tone:
- bronchial responsiveness naturally increases overnight, with peak airway narrowing between 3-4 AM.
🧪 Reduced cortisol levels:
- Our body's natural cortisol (which can be anti-inflammatory) dips during nighttime hours, potentially allowing more inflammation to occur.
🐩 Exposure to bedroom allergens:
- Dust mites, pet dander, and other allergens in bedding can exacerbate cough in sensitized individuals.
😝 Gastroesopheal reflux
- Lying flat can worsen reflux, and even small amounts of acid reaching the upper airway can trigger coughing through vagal stimulation.
The Historical Perspective:
From "Consumption" to Modern Understanding
Persistent coughing has plagued humanity for millennia.
Ancient Egyptian medical papyri from 1550 BCE describe treatments for lingering coughs using honey and herbs. Hippocrates wrote extensively about "katarrh" (catarrh), noting how respiratory symptoms could persist long after apparent recovery.
During the 18th and 19th centuries, persistent cough was often ominously associated with tuberculosis (then called "consumption").
This association created significant anxiety around any lingering cough—anxiety that persists in our collective medical consciousness even today especially since our Covid pandemic.
Hence the continued side eye 😒 when you’re coughing at the gym...
So what works to stop that cough?
Evidence-Based Management Strategies?
Honestly, not much.
It’s usually and mainly supportive care.
These have all been studied below.
- Inhaled ipratropium bromide has shown modest efficacy in reducing cough frequency in randomized controlled trials.
- Honey (for patients >2 years old) has evidence supporting its use, with studies showing it outperforms placebo for cough suppression.
- Dextromethorphan shows variable efficacy but may benefit a small set of patients.
- Intranasal steroids can be helpful, particularly if there's an allergic component.
- Gabapentin and pregabalin have emerging evidence for neuropathic or hypersensitivity-mediated cough, though they remain second-line options, but chronic cough is not our scope today.
- Capsaicin has been explored as its properties can stimulate the cough arc but also numb the reflex.
- Inhaled corticosteroids can work if there is substantial inflammation to the trachobrobchial tree.
Overall, treatments have less than 40% efficacy.
For patients managing this frustrating condition:
- Stay hydrated to maintain optimal mucus viscosity
- Use a humidifier to moisten airways, especially at night
- Elevate the head of your bed to minimize reflux and improve drainage
- Avoid irritants like cigarette smoke, strong perfumes, and pollution
- For adults, trial 1-2 tablespoons of honey, lemon, chili pepper, turmeric, and black pepper. That’s my mom’s recipe. 😃
- Be patient and understand the natural healing timeline of respiratory epithelium
Patience with Pathophysiology
Understanding the biological basis for persistent cough helps both doctors and patients navigate this common but frustrating condition.
While that 6-8 week timeline can seem interminable when you're coughing through that school or business presentation or even when struggling to sleep, knowing there's a physiological explanation and an endpoint can provide reassurance.
For our patients, we should explain that in most instances, antibiotic prescriptions may not be necessary. (Of course, each patient should be evaluated on a case by case basis.)
The next time you or your patient is dealing with that lingering cough, remember: your respiratory epithelium is hard at work rebuilding itself, and cilium by cilium.
Sometimes the best medicine is knowledge, patience, and a good night's sleep (propped up on a few extra pillows, of course).
References
- Dicpinigaitis PV. Post-viral cough: ACCP evidence-based clinical practice guidelines. Chest. 2006;129(1 Suppl):138S-146S.
- Irwin RS, French CL, Chang AB, Altman KW. Classification of Cough as a Symptom in Adults and Management Algorithms. Chest. 2018;153(1):196-209.
- Morice AH, McGarvey L, Pavord I. Recommendations for the management of cough in adults. Thorax. 2006;61(Suppl 1):i1-i24.
- Chung KF, Pavord ID. Prevalence, pathogenesis, and causes of chronic cough. Lancet. 2008;371(9621):1364-1374.
- Barnes PJ. Circadian variation in airway function. Am J Med. 1985;79(6A):5-9.
- O'Connell F, Thomas VE, Pride NB, Fuller RW. Capsaicin cough sensitivity decreases with successful treatment of chronic cough. Am J Respir Crit Care Med. 1994;150(2):374-380.
- Empey DW, Laitinen LA, Jacobs L, Gold WM, Nadel JA. Mechanisms of bronchial hyperreactivity in normal subjects after upper respiratory tract infection. Am Rev Respir Dis. 1976;113(2):131-139.
- Oduwole O, Meremikwu MM, Oyo-Ita A, Udoh EE. Honey for acute cough in children. Cochrane Database Syst Rev. 2014;(12):CD007094.
- Ryan NM, Birring SS, Gibson PG. Gabapentin for refractory chronic cough: a randomised, double-blind, placebo-controlled trial. Lancet. 2012;380(9853):1583-1589.
- Bonvini SJ, Birrell MA, Smith JA, Belvisi MG. Targeting TRP channels for chronic cough: from bench to bedside. Naunyn Schmiedebergs Arch Pharmacol. 2015;388(4):401-420.
- Chen L, Liu W, Zhang J, et al. Autonomic nervous system dysfunction in post-viral cough: heart rate variability analysis and clinical correlations. Respir Physiol Neurobiol. 2022;296:103801.
- Morice AH, Millqvist E, Bieksiene K, et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. Eur Respir J. 2020;55(1):1901136.
- Song WJ, Chang YS, Morice AH. Changing the paradigm for cough: does 'cough hypersensitivity' aid our understanding? Asia Pac Allergy. 2014;4(1):3-13.
- West PW, Canning BJ, Merlo-Pich E, et al. Neuroplasticity in models of the vagal innervation of the airways. Am J Respir Crit Care Med. 2023;207(3):284-292.
- Chang et al. Cough hypersensitivity syndrome. J Clinical Med. 2023.